Someone asked me today why my practice is better than the competition in providing cosmetic plastic surgery care; and that started me thinking.
Obviously I think that I am better than the other plastic surgeons in the area- otherwise why do I bother top get up in the morning? If I am truly caring physician, with my patient's best interest at heart, I should send them to someone else if I don't think that I am better!
By the time I finished training as a plastic surgeon I had already completed four years of college, a year of Masters studies in physiology, four years of medical school, five years of general surgery training and three years of plastic surgery training- 17 years after high school. Only then did I start to learn.
I became technically proficient with my training and was board certified. It took another ten years to become truly an expert in cosmetic surgery. Some types of plastic surgery I stopped performing years ago; for the past ten years I have limited my practice to only cosmetic surgery; breast enlargements,lifts and reductions,tummy tucks,face lift, rhinoplasty, eyelids surgery, liposuction. I have continued to learn new techniques in plastic surgery, and to shy away from untested hype. But is that enough; to be an expert surgeon in my field?
NO- I think that I am better than my colleagues because apart form the advanced techniques that I use, I also provide extraordinary care for my patients, and that is why I get superb results. I like my patients; and I treat them as if they were my family; my wife, my mother, my sister or brother, father, son or daughter. Once you do that you are sure that you have always done your best. The excellence then just follows naturally.
Monday, October 11, 2010
Sunday, June 20, 2010
The Latest Plastic Surgery news of 2010
Plastic surgery techniques -2010
The American Society of Plastic Surgeons held its annual meeting in Washington, D.C. last month.
Over 4000 plastic surgeons from around the world attended this meeting bringing ideas and techniques from all over the world- some superb, some pathetic!
Here I will give you a synopsis of the latest techniques in plastic surgery as of 2010, and what I learnt at the meeting; techniques are classified as having UNKNOWN EFFICAY, are REJECTED or ACCEPTED as being beneficial for patients.
THERMAGE, a technique where energy is transferred to the skin for tightening, instead of a facelift, is overwhelmingly REJECTED. There are hundreds of these machines on sale in the second hand market from surgeons who bought, tried, and were unhappy with their results nearly as much as their patients.
THREADLIFTS, LIFESTYLE lifts or any variation of face lifting by percutaneous sutures is REJECTED. The companies promoting these types of surgery are essentially marketing companies headed by non plastic surgeons, and are trying to dupe patients into having their procedures with mis leading photos (most of the patients have had other procedures also). Some studies show that almost 80% of patients are dissatisfied with their results- typically, results that last a year only. The companies are also aggressively pursuing surgeons who speak against their “procedures” in a legal manner. Beware of these techniques!!
FAT GRAFTING to the face and buttocks is ACCEPTED.
Fat grafting to the breast has UNKNOWN EFFICACY- Fat grafting to the breast became fashionable a few years ago after years of it being a medical taboo. The fat injected to the breast calcified and was often mistaken for a cancer of the breast on mammograms. Over the years mammography techniques improved and radiologist could decipher between the calcifications due to fat necrosis and true cancer of the breast. Plastic surgeons became emboldened and began injecting fat into the breast to achieve breast enlargement; usually of just one cup size at most, and then with need for suction cups on the breast for at least 8 hours a day etc.. At the latest meeting however the technique has become very controversial given that some animal studies showed an increase in cancer of the breast when injected with fat . So , I'm going to wait on this one.
MESOTHERAPY, a technique where chemicals are injected into the skin to destroy fat cells and hence remove fat has UNKNOWN EFFICACY . This is the technique that refuses to die. Popular a few years ago, with numerous spas advertising the miracle fat dissolving injections, the technique was taken off the market after numerous complaints from unsatisfied patients who had paid thousands of dollars for a technique that did not work. The researchers have gone “back to the drawing board” to see if they can come up with a better technique. So, I'm going to wait on this one.
SCULPTRA is ACCEPTED. I have been using Sculptra for several years with excellent results for filling the face and increasing the facial volume. Probably the greatest mistake I have made is not injecting enough of the material ! Since its approval for cosmetic use this material has come into its own.
EVOLENCE has UNKNOWN EFFICAY. Studies are underway to determine the side effects of this new permanent material for facial line injections. The small particles of poly methyl methacralate will stay in the body, where they are injected, for ever. But, the body keeps on moving ,so the surgeon has to be careful as to where and how it is injected.
LASER LIPOSUCTION is REJECTED as being more of a gimmick than anything else. Overwhelmingly, surgeons at the conference voted for viewing the results of laser liposuction as being no different than any other type of liposuction. Another marketing technique being used by companies to sell the public on unnecessary techniques and technologies for their profit.
ANTIBIOTICS; Giving antibiotics 30mins before the surgery is very important and ACCEPTED. Prophylactic antibiotics are being overused and when they are used are being given too early or too late, a recent study showed. I have changed my practice in view of this finding. The rate of infections is halved by giving the antibiotic at the correct time.
WARMING BLANKETS: Keeping the patient warm before and during the surgery to decrease rate of infections is ACCEPTED. Not only is the infection rate less, but patients will recover faster from anesthesia also!
These were just some of the highlights of the meeting that stood out; I am glad I was able to share them with you.
Please call or email me at www.tavmd.com me if you need more information or have any questions!
The American Society of Plastic Surgeons held its annual meeting in Washington, D.C. last month.
Over 4000 plastic surgeons from around the world attended this meeting bringing ideas and techniques from all over the world- some superb, some pathetic!
Here I will give you a synopsis of the latest techniques in plastic surgery as of 2010, and what I learnt at the meeting; techniques are classified as having UNKNOWN EFFICAY, are REJECTED or ACCEPTED as being beneficial for patients.
THERMAGE, a technique where energy is transferred to the skin for tightening, instead of a facelift, is overwhelmingly REJECTED. There are hundreds of these machines on sale in the second hand market from surgeons who bought, tried, and were unhappy with their results nearly as much as their patients.
THREADLIFTS, LIFESTYLE lifts or any variation of face lifting by percutaneous sutures is REJECTED. The companies promoting these types of surgery are essentially marketing companies headed by non plastic surgeons, and are trying to dupe patients into having their procedures with mis leading photos (most of the patients have had other procedures also). Some studies show that almost 80% of patients are dissatisfied with their results- typically, results that last a year only. The companies are also aggressively pursuing surgeons who speak against their “procedures” in a legal manner. Beware of these techniques!!
FAT GRAFTING to the face and buttocks is ACCEPTED.
Fat grafting to the breast has UNKNOWN EFFICACY- Fat grafting to the breast became fashionable a few years ago after years of it being a medical taboo. The fat injected to the breast calcified and was often mistaken for a cancer of the breast on mammograms. Over the years mammography techniques improved and radiologist could decipher between the calcifications due to fat necrosis and true cancer of the breast. Plastic surgeons became emboldened and began injecting fat into the breast to achieve breast enlargement; usually of just one cup size at most, and then with need for suction cups on the breast for at least 8 hours a day etc.. At the latest meeting however the technique has become very controversial given that some animal studies showed an increase in cancer of the breast when injected with fat . So , I'm going to wait on this one.
MESOTHERAPY, a technique where chemicals are injected into the skin to destroy fat cells and hence remove fat has UNKNOWN EFFICACY . This is the technique that refuses to die. Popular a few years ago, with numerous spas advertising the miracle fat dissolving injections, the technique was taken off the market after numerous complaints from unsatisfied patients who had paid thousands of dollars for a technique that did not work. The researchers have gone “back to the drawing board” to see if they can come up with a better technique. So, I'm going to wait on this one.
SCULPTRA is ACCEPTED. I have been using Sculptra for several years with excellent results for filling the face and increasing the facial volume. Probably the greatest mistake I have made is not injecting enough of the material ! Since its approval for cosmetic use this material has come into its own.
EVOLENCE has UNKNOWN EFFICAY. Studies are underway to determine the side effects of this new permanent material for facial line injections. The small particles of poly methyl methacralate will stay in the body, where they are injected, for ever. But, the body keeps on moving ,so the surgeon has to be careful as to where and how it is injected.
LASER LIPOSUCTION is REJECTED as being more of a gimmick than anything else. Overwhelmingly, surgeons at the conference voted for viewing the results of laser liposuction as being no different than any other type of liposuction. Another marketing technique being used by companies to sell the public on unnecessary techniques and technologies for their profit.
ANTIBIOTICS; Giving antibiotics 30mins before the surgery is very important and ACCEPTED. Prophylactic antibiotics are being overused and when they are used are being given too early or too late, a recent study showed. I have changed my practice in view of this finding. The rate of infections is halved by giving the antibiotic at the correct time.
WARMING BLANKETS: Keeping the patient warm before and during the surgery to decrease rate of infections is ACCEPTED. Not only is the infection rate less, but patients will recover faster from anesthesia also!
These were just some of the highlights of the meeting that stood out; I am glad I was able to share them with you.
Please call or email me at www.tavmd.com me if you need more information or have any questions!
Monday, November 10, 2008
Beauty and Plastic surgery
Almost on a daily basis I ask myself the relationship between beauty and what I, as a plastic surgeon performing cosmetic operations, do. I ask myself did I achieve a beautiful result; did I make the patient look “younger”, “more rested”, more beautiful? The more years I am in practice, the more I understand this relationship between our perceptions of beauty and what I do surgically or by other interventions to enhance that idea.
The surprising conclusion I have reached is summed up in one word; Normal.
The best results that I can possibly achieve are where the patient looks normal! That is to say that my patient has no physical characteristics that stand out to such an extent that allow you, the observer, to identify, classify or remark on. In essence, and contrary to commonly held modern beliefs about our uniqueness and individuality, when it comes to our looks we all just want to be normal; with unimpeachable physical characteristics.
As humans we have a tendency to identify each other by physical characteristics. The most obvious and nefarious has been skin color along with its well known historical and social sequelae. But even after color we keep on separating and identifying each other by the size and shape of our nose, breasts, body, ears, hair, eyes, and so on. How many times has someone tried to identify another as “ the normal height and weight white girl with normal breasts and normal eyes, ears and nose, and with no scars.” A much more common identifier is” the short, fat, black man with big breasts and a hooked nose with floppy ears, droopy eyelids, and a scar on his face”. (Guess what? Almost all these characteristics can be improved by plastic surgery! )
In a reverse anthropomorphism, we identify other humans by the physical characteristics that set them apart from the rest of the herd. “Ugliness” can hence be defined as physical characteristics and deformities that fall outside of the perceived social norm for that group, in that particular time period, and by which an individual can be identified as being other. But does the inverse definition apply to our concept of beauty?
That is physical characteristics that are at the middle of the norm of the group for a particular period? Surely we do not mean that the most “plain Jane” is the most beautiful? The girl or boy that we cannot describe in any way? Well, try it- think of a beautiful woman of our times; try to describe her. It is difficult. Yet we all have a very similar concept of what makes a human “beautiful”, hard wired into our brains, even if we cannot put it into words. That concept may change somewhat over time with new fashions and styles, but the basis is the same across races and history. Physical beauty ends up meaning that we find a certain harmony in the characteristics we are looking at, be they a whole body, a face, a hand, or even a nose.
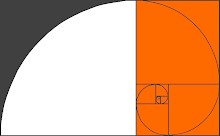
The Golden mean or ratio ( 1:1.618) is a mathematical ratio found throughout nature that relates differing parts of natural objects to one another. This is one ratio that we find beautiful; this is one of those harmonies we seek. For example the length of the eyelid (1) to the length of the mouth (1.618) is though by most to be beautiful. Likewise, the width of the front incisor tooth (1.618) to the tooth directly next to it(1). The list goes on ad infinitum.
Apart from these “hard wired” perceptions of beauty, there are other “ hard wired” criteria by which we also judge each other’s appearance.
For example, we are pre-programmed to look for and notice objects that are dark and round. They attract our attention much more than, say, a dark line. This ability rests on a species recognition trait that allows us to recognize each other as being from a similar life form as opposed to a lizard. Our pupils, out nipples, belly buttons, are all round and dark for that reason. In fact, during the 18th century both men and women of means and fashion used this innate ability of our brains to attract attention to themselves by the use of applied beauty marks, mimicking skin moles.
The quality of the skin is also one such criterion. Even if one’s bone structure and relations of nose to mouth are not in the golden mean proportion, should we have a clear complexion with smooth skin, we are thought of as being more attractive. The answer to this is that we are programmed to beware of outward (skin and body) signs of disease in those around us. It’s a warning mechanism with its basis as the suitability of the individual as a sexual partner. For example, if your neighbor has pimples and pustules, skin discoloration, unevenness of the texture, or peeling skin, you are apt to keep your distance and avoid contact lest you catch their illness. God forbid that they have wrinkles, moles, or other growths on the skin that are giveaways for being older (and less attractive for procreation)- Just close your eyes and imagine a witch. Do you see her warty growths on her nose and chin?
The converse, clear skin that is smooth and free of blemishes, alludes to a healthy young person who is sexually more attractive.
A multi-billion dollar cosmetic industry exists worldwide to counter our innate ability to discern. Cosmetic surgery is also part of this collusion against our primitive instincts of judging each other by our physical characteristics. It makes the playing field more even and allows our intellect the opportunity to shine through our body coverings. Plastic surgery procedures allow the unsightly conversation pieces that our bodies may provide, to be transformed and disappear. It’s that change that we see in ourselves when looking in a mirror, and that others see when looking at us, that changes attitudes from within and from the outside.
Beauty is truly in the eye of the beholder, but it seems we are all looking through the same lens at different periods of history. Also, we all know that the eye can be tricked by the sleight of hand (with a scalpel).
The surprising conclusion I have reached is summed up in one word; Normal.
The best results that I can possibly achieve are where the patient looks normal! That is to say that my patient has no physical characteristics that stand out to such an extent that allow you, the observer, to identify, classify or remark on. In essence, and contrary to commonly held modern beliefs about our uniqueness and individuality, when it comes to our looks we all just want to be normal; with unimpeachable physical characteristics.
As humans we have a tendency to identify each other by physical characteristics. The most obvious and nefarious has been skin color along with its well known historical and social sequelae. But even after color we keep on separating and identifying each other by the size and shape of our nose, breasts, body, ears, hair, eyes, and so on. How many times has someone tried to identify another as “ the normal height and weight white girl with normal breasts and normal eyes, ears and nose, and with no scars.” A much more common identifier is” the short, fat, black man with big breasts and a hooked nose with floppy ears, droopy eyelids, and a scar on his face”. (Guess what? Almost all these characteristics can be improved by plastic surgery! )
In a reverse anthropomorphism, we identify other humans by the physical characteristics that set them apart from the rest of the herd. “Ugliness” can hence be defined as physical characteristics and deformities that fall outside of the perceived social norm for that group, in that particular time period, and by which an individual can be identified as being other. But does the inverse definition apply to our concept of beauty?
That is physical characteristics that are at the middle of the norm of the group for a particular period? Surely we do not mean that the most “plain Jane” is the most beautiful? The girl or boy that we cannot describe in any way? Well, try it- think of a beautiful woman of our times; try to describe her. It is difficult. Yet we all have a very similar concept of what makes a human “beautiful”, hard wired into our brains, even if we cannot put it into words. That concept may change somewhat over time with new fashions and styles, but the basis is the same across races and history. Physical beauty ends up meaning that we find a certain harmony in the characteristics we are looking at, be they a whole body, a face, a hand, or even a nose.
The Golden mean or ratio ( 1:1.618) is a mathematical ratio found throughout nature that relates differing parts of natural objects to one another. This is one ratio that we find beautiful; this is one of those harmonies we seek. For example the length of the eyelid (1) to the length of the mouth (1.618) is though by most to be beautiful. Likewise, the width of the front incisor tooth (1.618) to the tooth directly next to it(1). The list goes on ad infinitum.
Apart from these “hard wired” perceptions of beauty, there are other “ hard wired” criteria by which we also judge each other’s appearance.
For example, we are pre-programmed to look for and notice objects that are dark and round. They attract our attention much more than, say, a dark line. This ability rests on a species recognition trait that allows us to recognize each other as being from a similar life form as opposed to a lizard. Our pupils, out nipples, belly buttons, are all round and dark for that reason. In fact, during the 18th century both men and women of means and fashion used this innate ability of our brains to attract attention to themselves by the use of applied beauty marks, mimicking skin moles.
The quality of the skin is also one such criterion. Even if one’s bone structure and relations of nose to mouth are not in the golden mean proportion, should we have a clear complexion with smooth skin, we are thought of as being more attractive. The answer to this is that we are programmed to beware of outward (skin and body) signs of disease in those around us. It’s a warning mechanism with its basis as the suitability of the individual as a sexual partner. For example, if your neighbor has pimples and pustules, skin discoloration, unevenness of the texture, or peeling skin, you are apt to keep your distance and avoid contact lest you catch their illness. God forbid that they have wrinkles, moles, or other growths on the skin that are giveaways for being older (and less attractive for procreation)- Just close your eyes and imagine a witch. Do you see her warty growths on her nose and chin?
The converse, clear skin that is smooth and free of blemishes, alludes to a healthy young person who is sexually more attractive.
A multi-billion dollar cosmetic industry exists worldwide to counter our innate ability to discern. Cosmetic surgery is also part of this collusion against our primitive instincts of judging each other by our physical characteristics. It makes the playing field more even and allows our intellect the opportunity to shine through our body coverings. Plastic surgery procedures allow the unsightly conversation pieces that our bodies may provide, to be transformed and disappear. It’s that change that we see in ourselves when looking in a mirror, and that others see when looking at us, that changes attitudes from within and from the outside.
Beauty is truly in the eye of the beholder, but it seems we are all looking through the same lens at different periods of history. Also, we all know that the eye can be tricked by the sleight of hand (with a scalpel).
0
comments
Labels:
artefill,
beauty,
cosmetic surgery,
golden mean,
nature,
plastic surgery,
proportion


Saturday, November 10, 2007
Lessons we should learn from the case of Dr. Jan Adams and Mrs.West.
The unfortunate case of Mrs. West's death following breast reduction and abdominoplasty by Dr. Jan Adams, in California has generated many questions and intense scrutiny in the Press and from Patients. As in many of these unfortunate types of cases, there are many lessons to be learnt and currently the Press is ignoring the truly important aspects that need to be discussed.
Let me make a disclaimer. I know Dr. Adams personally, as we were co-residents in General Surgery during five years of training at Lenox Hill Hospital in New York City. I have seen Dr. Adams operate and take care of his patients first hand- most plastic surgeons cannot make this claim with respect to their colleagues. Dr. Adams is a great surgeon- he is intelligent, educated, articulate, and exceptionally well trained as a plastic surgeon at some of the premier institutions in this country, and is technically gifted. (Many surgeons are fumblers-believe it or not!)
From what I can gather, Mrs. West was an equally intelligent, well informed middle aged women with minor medical conditions which many patients have and which would not exclude anyone from undergoing cosmetic surgery.
Complications can occur in any surgical procedure and though death is extremely rare, it is obviously what all patients and surgeons at least think about, however fleetingly, as a possibility at some point during the consultation, surgery set up period, during the surgery or in the post-operative period. It is the "unspeakable but not the mentionable" risk that exists with any surgical procedure. What the cause of Mrs. West's demise was, will hopefully be made clear after tests are done. One thing that is already clear to any surgeon is that Dr. Adams did not kill Mrs. West, as has been insinuated in the Press and TV.
The fact that Dr. Adams is not a board certified plastic surgeon does not have any relation to the case. He was trained as a plastic surgeon and has been practicing as one for over 15 years. MANY THOUSANDS OF PLASTIC SURGEONS ARE NOT BOARD CERTIFIED - BUT THEY ARE PLASTIC SURGEONS. There are numerous reasons why a plastic surgeon may not become board certified and almost all are due to politics within the Plastic surgery community, or personal reasons on the part of the surgeon. To think that a candidate for board certification in plastic surgery, after going through some of the most rigorous training offered in medicine and surgery, after having taken literally thousands of exams, and risen above his or her competitors during high school, college, medical school and residency training, should somehow not be performing plastic surgery is nonsense.
The real issue that we should be focusing on and for which a national discussion is long overdue is the fact that the majority of cosmetic surgery procedures in this country are performed by doctors who are not trained plastic surgeons, and in many cases, not even surgeons. There are about 450,000 doctors in this country and 60,000 doctors who perform cosmetic surgery- yet there are only 6000 plastic surgeons- and of those, only about 3000 are members of the American Society for Aesthetic Plastic Surgery- plastic surgeons who perform cosmetic surgery primarily.
The vast number of cosmetic surgeries are being performed by doctors who are untrained in plastic surgery. They may be board certified, but are board certified in disciplines other than plastic surgery. Plastic surgeons typically have trained for 6-8 years after medical school. They are dermatologists ( with a one month training as a junior resident on a surgical team as part of their 3 years of dermatology training), gynecologists / obstetricians (whose area of expertise is obviously limited to certain anatomical areas during their 4-5 years of training), general surgeons (who do not take the extra 2-3 years of training needed to become a plastic surgeon after a 5 year general surgery training), Ear nose throat (ENT) surgeons - 4 years training-who call themselves facial plastic surgeons yet somehow manage to include the whole body in the ear/nose/throat area!), and even doctors such as anesthesiologists and internists, who have barely ever held a scalpel, and now days even dentists are doing facelifts!
Why does this happen?... and this is the shocker - because they can! Any physician receives from their state a license to practice Medicine and Surgery. The License is not restrictive in any sense within the boundries of Medicine and Surgery. Any doctor can do anything! Theoretically nothing prevents me from performing brain surgery on a patient- even though I am not a trained brain surgeon- all I need is a patient who will let me operate on them - and imagine that I tell them that "I am board certified" (as I am in Plastic surgery but not Neurosurgery). They would think that the state or federal government has qualified me to perform the brain surgery I am proposing! and how wrong they would be.
So why do so many doctors perform plastic and cosmetic surgery without being trained to do them? Because they figure that the risks of plastic surgery and cosmetic procedures are low enough that they can risk a complication for the economic gains they get; and should they get a complication, nothing in the law says they could not do that procedure!
Are the doctors doing cosmetic surgery cheaper than the plastic surgeons? No! In some cases they even charge more for the same procedure than a qualified surgeon- it’s pure ignorance on the part of the public- and license laws that are arcane.
The threat to public safety is not from plastic surgeons that have been trained and are not board certified in Plastic surgery: the threat is from doctors who are not trained in plastic surgery and "board certified" in other disciplines.
Let me make a disclaimer. I know Dr. Adams personally, as we were co-residents in General Surgery during five years of training at Lenox Hill Hospital in New York City. I have seen Dr. Adams operate and take care of his patients first hand- most plastic surgeons cannot make this claim with respect to their colleagues. Dr. Adams is a great surgeon- he is intelligent, educated, articulate, and exceptionally well trained as a plastic surgeon at some of the premier institutions in this country, and is technically gifted. (Many surgeons are fumblers-believe it or not!)
From what I can gather, Mrs. West was an equally intelligent, well informed middle aged women with minor medical conditions which many patients have and which would not exclude anyone from undergoing cosmetic surgery.
Complications can occur in any surgical procedure and though death is extremely rare, it is obviously what all patients and surgeons at least think about, however fleetingly, as a possibility at some point during the consultation, surgery set up period, during the surgery or in the post-operative period. It is the "unspeakable but not the mentionable" risk that exists with any surgical procedure. What the cause of Mrs. West's demise was, will hopefully be made clear after tests are done. One thing that is already clear to any surgeon is that Dr. Adams did not kill Mrs. West, as has been insinuated in the Press and TV.
The fact that Dr. Adams is not a board certified plastic surgeon does not have any relation to the case. He was trained as a plastic surgeon and has been practicing as one for over 15 years. MANY THOUSANDS OF PLASTIC SURGEONS ARE NOT BOARD CERTIFIED - BUT THEY ARE PLASTIC SURGEONS. There are numerous reasons why a plastic surgeon may not become board certified and almost all are due to politics within the Plastic surgery community, or personal reasons on the part of the surgeon. To think that a candidate for board certification in plastic surgery, after going through some of the most rigorous training offered in medicine and surgery, after having taken literally thousands of exams, and risen above his or her competitors during high school, college, medical school and residency training, should somehow not be performing plastic surgery is nonsense.
The real issue that we should be focusing on and for which a national discussion is long overdue is the fact that the majority of cosmetic surgery procedures in this country are performed by doctors who are not trained plastic surgeons, and in many cases, not even surgeons. There are about 450,000 doctors in this country and 60,000 doctors who perform cosmetic surgery- yet there are only 6000 plastic surgeons- and of those, only about 3000 are members of the American Society for Aesthetic Plastic Surgery- plastic surgeons who perform cosmetic surgery primarily.
The vast number of cosmetic surgeries are being performed by doctors who are untrained in plastic surgery. They may be board certified, but are board certified in disciplines other than plastic surgery. Plastic surgeons typically have trained for 6-8 years after medical school. They are dermatologists ( with a one month training as a junior resident on a surgical team as part of their 3 years of dermatology training), gynecologists / obstetricians (whose area of expertise is obviously limited to certain anatomical areas during their 4-5 years of training), general surgeons (who do not take the extra 2-3 years of training needed to become a plastic surgeon after a 5 year general surgery training), Ear nose throat (ENT) surgeons - 4 years training-who call themselves facial plastic surgeons yet somehow manage to include the whole body in the ear/nose/throat area!), and even doctors such as anesthesiologists and internists, who have barely ever held a scalpel, and now days even dentists are doing facelifts!
Why does this happen?... and this is the shocker - because they can! Any physician receives from their state a license to practice Medicine and Surgery. The License is not restrictive in any sense within the boundries of Medicine and Surgery. Any doctor can do anything! Theoretically nothing prevents me from performing brain surgery on a patient- even though I am not a trained brain surgeon- all I need is a patient who will let me operate on them - and imagine that I tell them that "I am board certified" (as I am in Plastic surgery but not Neurosurgery). They would think that the state or federal government has qualified me to perform the brain surgery I am proposing! and how wrong they would be.
So why do so many doctors perform plastic and cosmetic surgery without being trained to do them? Because they figure that the risks of plastic surgery and cosmetic procedures are low enough that they can risk a complication for the economic gains they get; and should they get a complication, nothing in the law says they could not do that procedure!
Are the doctors doing cosmetic surgery cheaper than the plastic surgeons? No! In some cases they even charge more for the same procedure than a qualified surgeon- it’s pure ignorance on the part of the public- and license laws that are arcane.
The threat to public safety is not from plastic surgeons that have been trained and are not board certified in Plastic surgery: the threat is from doctors who are not trained in plastic surgery and "board certified" in other disciplines.
Tuesday, October 30, 2007
The Latest trend in Breast Augmentation
This week I attended the annual meeting of the American Society of Plastic Surgeons, the national organization to which all board certified and eligible Plastic surgeons can belong,in Baltimore, Maryland.
This conference and others like it which I attend regularly, provides not only an opportunity to discuss with colleagues their techniques for surgery, the chance to see the latest tools and gadgets for plastic surgery, but also an educational opportunity to learn new techniques that are being proposed.
Last year saw the FDA approval of silicone breast implants and their re-introduction into the US market after 15 years of restricted use. Currently only 16-18 % of breast implants in the US are being performed with silicone implants. The majority of patients and surgeons still prefer the saline implants. Last week a new technique for breast augmentation using the patient’s own fat was proposed as being an alternative for some patients.
Fat has always been thought of as the ideal breast augmentation material since the breast itself is mainly made of fat in any case. With a breast enlargement with fat, there would be no foreign implants or the risks associated with such. However, Plastic surgeons have been taught for decades that fat injection into the breasts is not a choice in breast augmentation as the fat would lead to micro-calcifications over time that could be confused with the type of calcifications seen with breast cancer. This was then thought to lead to many women having unnecessary breast biopsies and having to deal with the ordeal of a possible breast cancer.
Now it seems, that the techniques for identification of calcifications on mammograms have improved that there seems to be no confusion between a benign fatty calcification and the type caused by cancer. Fat injection into the breast is now being studied as an alternative to breast augmentation with implants.
From my experience with fat injections into the face and buttocks I already know that when injected, some fat will die and be re-absorbed into the body. The skill of the surgeon, technique used, amount of fat used and its preparation are all factors that affect the survival of the fat grafts. However it is safe to assume that some fat will remain and that the breast enlargement will be permanent to some degree. I would suspect that initially this is would be a good method for patients who would otherwise be candidates for smaller implants. Of course, patients need to have sufficient amounts of fat to be liposuctioned before any can be injected and should realize that multiple (2-3) procedures may be necessary. Patients who are considering this technique can contact me for more information.
This conference and others like it which I attend regularly, provides not only an opportunity to discuss with colleagues their techniques for surgery, the chance to see the latest tools and gadgets for plastic surgery, but also an educational opportunity to learn new techniques that are being proposed.
Last year saw the FDA approval of silicone breast implants and their re-introduction into the US market after 15 years of restricted use. Currently only 16-18 % of breast implants in the US are being performed with silicone implants. The majority of patients and surgeons still prefer the saline implants. Last week a new technique for breast augmentation using the patient’s own fat was proposed as being an alternative for some patients.
Fat has always been thought of as the ideal breast augmentation material since the breast itself is mainly made of fat in any case. With a breast enlargement with fat, there would be no foreign implants or the risks associated with such. However, Plastic surgeons have been taught for decades that fat injection into the breasts is not a choice in breast augmentation as the fat would lead to micro-calcifications over time that could be confused with the type of calcifications seen with breast cancer. This was then thought to lead to many women having unnecessary breast biopsies and having to deal with the ordeal of a possible breast cancer.
Now it seems, that the techniques for identification of calcifications on mammograms have improved that there seems to be no confusion between a benign fatty calcification and the type caused by cancer. Fat injection into the breast is now being studied as an alternative to breast augmentation with implants.
From my experience with fat injections into the face and buttocks I already know that when injected, some fat will die and be re-absorbed into the body. The skill of the surgeon, technique used, amount of fat used and its preparation are all factors that affect the survival of the fat grafts. However it is safe to assume that some fat will remain and that the breast enlargement will be permanent to some degree. I would suspect that initially this is would be a good method for patients who would otherwise be candidates for smaller implants. Of course, patients need to have sufficient amounts of fat to be liposuctioned before any can be injected and should realize that multiple (2-3) procedures may be necessary. Patients who are considering this technique can contact me for more information.
Subscribe to:
Posts (Atom)